
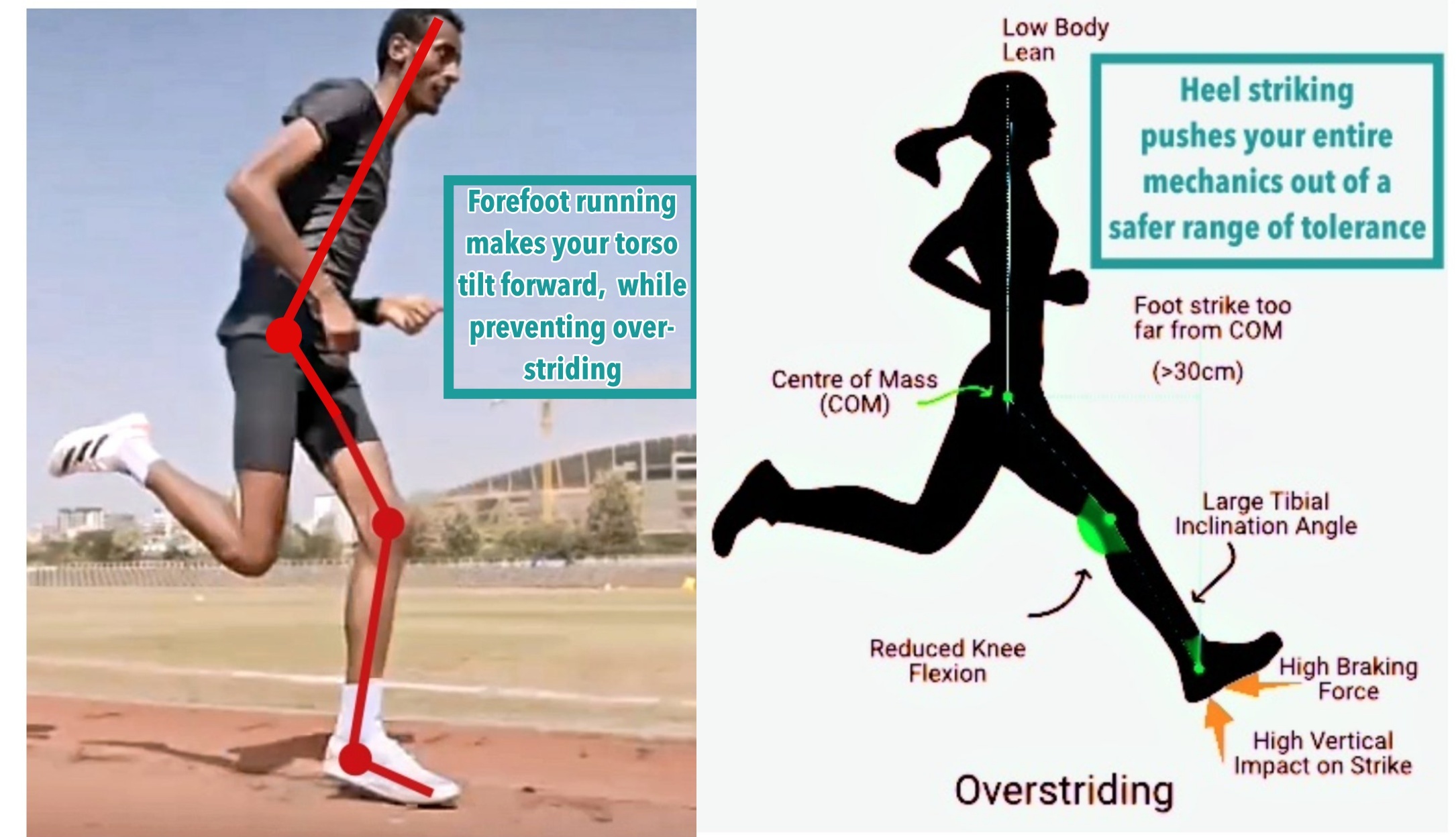
Heel strike running is the only running style that produces an assortment of impact forces that the muscles, and even the thickest cushioned running shoe cannot absorb. So, what are the benefits to that? None. Which is why there’s a big, ongoing interest in other running styles, like forefoot running (see here what a proper forefoot strike looks like).
In fact, the impacts produced in heel strike running are so severe that they damage the nerves, resulting in nerve injuries.


In running, nerve injuries are the result of regular exposure to high repetitions of high impact motions, high muscular forces and extreme foot positions [1], all of which are common traits of heel strike running, but not in forefoot running.
For a side note, optimal nerve health has a strong structural basis:
- conduction velocity (speed of signal) is proportional to the diameter of the nerve fiber whereby soft tissue swelling perturbs the geometry of a nerve cell, interfering with conduction
- because a signal cannot pass strongly and stably under these conditions, movement efficiency is compromised and peripheral neuropathy may result [2]
Unlike forefoot running, heel strike running produces a number of enormous, more immediate impacts that directly cause nerve injuries, such as nerve entrapment. The specific heel strike-related forces are patellofemoral (knee) and tibiofemoral (shin) compressive forces, intramuscular compartmental pressures, impact peaks and ground reaction forces as well as more overall mechanical loading on the musculoskeletal system [3-7].


Moreover, the adverse effects of heel strike running on peripheral nerve function surfaced in a study by Colak et al. [3]
- The researchers examined and compared motor conduction velocities of the tibial and peroneal nerve and sensory conduction velocities of the medial and lateral plantar nerve, the sural and superficial peroneal nerve in habitual shod (shoe) runners and non-runners (heel strike running is associated with habitual shod running*).
The researchers found that the habitual shod runners had delayed sensory conduction velocities in the lateral and medial plantar nerves as well as the sural nerve compared to the non-runners.
Interestingly, the researchers were shocked to find that running effected the sural nerve since isolated sural nerve injuries are rare. Likewise, it comes as no surprise that sural nerve function was impaired given the magnitude of bone strain cycles and relative greater loads associated with heel strike running.
Regain Nerve Function with Forefoot Running

Humans evolved to use the same basic networks of brain parts and peripheral nerves that control basic motor parts for running barefoot that is. Humans also evolved to use the same foot strike during running -the forefoot strike, which has been disrupted by the modern running shoe which causes us to heel strike due to the elevated heel of these shoes.
Because of the thick underfoot cushioning and narrow, inflexible fit, the conventional running shoe impairs the natural tendency to follow what the feet feel during running, causing us to use abnormal foot mechanics (i.e. heel strike) that generate more impact. Researchers agree that running shoes with thickly, cushioned heels facilitates heel strike, and by running barefoot or at least in barefoot-inspired shoe, a forefoot strike, and therefore low impact mechanics, can be easily maintained.
In this regard, forefoot running cuts down on skeletal loading and thus, does not interfere with the all the factors that influence healthy nerve function.
On that note, here are all the evidence-backed reasons forefoot running works and heel strike running hurts. Here are also proven reason barefoot running can make you run better all-around in shoes!

If you’ve enjoyed my post, you’ll love my YouTube channel, here, where I show why forefoot running is the safest, most efficient way to run, and why heel strike running is very self-defeating!
References:
[1]. Banarjee T, Koons DD. Superficial peroneal nerve entrapment: Report of two cases. J Neuro Surg 1981, 55:991-992.
[2]. Rask MR. Medial plantar neuropraxia Jogger’s foot): Report of 3 cases, Clin Orthop 1978, 134:193-195.
[3]. Colak et al. Comparison of nerve conduction velocities of lower extremities between runners and controls. J Sci Med Sport, 2005; 8(4):403-410.
[4]. Aminoff MJ. Tibial and sural neuropathies. In : Electromyography in Clinical Practice. 3 rd Ed. Churchill Livingstone. P 479-492.1998.
[5]. Jackson DL, Haglund B. Tarsal tunnel syndrome in athletes. Am J Sports Med 1991;19:61- 65.
[6]. Jackson DL, Haglund B. Tarsal tunnel syndrome in runners. Sports Med 1992; 13:146-149. Henricson AS, Westin NE. Chronic calcaneal pain in athletes: Entrapment of the calcaneal nerve? Am J Sports Med 1984; 12:152-54.
[7]. Leach RE, Purnell MB, Saito A. Peroneal nerve entrapment in runners. Am J Sports Med 1989; 17:287-291.

If you’d like, you can support Run Forefoot and help keep it going by making a donation in any amount of your choosing:

Or, you can support Run Forefoot by shopping at the BEST Barefoot Shoe Brands, and be sure to bookmark these links 🙂
Lonowear: https://lonowear.com/?ref=cedsholh
Saguaro: https://www.saguaro.com/?ref=9bVA8fEkmDvB-I
Vibram FiveFingers: https://amzn.to/3VQLAUI
Vivobarefoot: https://amzn.to/3vycQOY
Be Lenka: https://www.tkqlhce.com/click-7600968-13947200
Xero Shoes: https://xeroshoes.com/go/Run_Forefoot
Iguaneye: https://www.iguaneye.com/?ref=8tfXVc92
Soft Star Shoes: https://shrsl.com/3mp1b
Wilding Shoes: https://bit.ly/3lIygQP
Sandra,Thank you for your post. It reminded me that patients and healthcrae providers alike often need to be reminded of the importnat differences between addiction, psuedoaddiction, physical dependence, and tolerance. I have uploaded a table for readers to review this. It may be found here,
It’s great to find an expert who can explain things so well